The Realities of Front‑Line Eye Care in Underserved Communities: A Portable Lumio Case Study
Across many parts of the world, access to portable eye care remains limited, and for too many people, preventable vision loss becomes a lived reality. Aston Vision Sciences donated the Lumio device to Al‑Shifa Trust Eye Hospital, the first dedicated eye hospital in Islamabad, serving not only the city but also a wide network of surrounding villages and farms with the intention of providing portable eye care to underserved communities.
What follows reflects my day‑to‑day experience working on the front line of eye care—both in hospital clinics and in remote outreach settings—and how Lumio has changed what we are able to offer our patients.
At a glance:
| Challenge: | How to reach patients that in remote communities when traditional equipment is non-portable and there are over 500 eye tests you need to conduct per day? |
| Environment: | Outreach/ Bush Clinics in rural Pakistan, Islamabad region. |
| Results: |
|
Patient numbers and populations
As the first eye hospital in Islamabad, we serve a very large and diverse population, including people from nearby rural villages and agricultural communities.
On routine hospital screening days, we typically see around 80–100 patients per day. Our patients range across all age groups, from young children to elderly adults, and many present with a high burden of preventable or untreated eye disease, largely due to limited access to specialist eye care.
In addition to hospital services, we regularly conduct outreach eye camps, usually located one to two hours’ travel from the hospital. During these camps, we may screen up to 600 patients in a single day. Outreach work mainly focuses on vision screening, the provision of glasses, and cataract screening, typically using an ophthalmoscope and, when possible, dilating drops.
Common eye conditions we encounter
We see a wide range of pathology. Common presentations include viral eye disease, such as herpes, ocular trauma, and foreign bodies, which are particularly frequent during the harvest season. Environmental exposure and occupational risks play a significant role in many of these cases.
Overall, we see a high prevalence of environment‑ and work‑related eye disease, alongside a large amount of unmet need for basic eye care. Many people who suffer an eye injury but live far from the hospital hope, believe they can simply “walk off” an eye condition. Unfortunately, this delay can be very dangerous and often leads to more serious complications by the time they finally seek help.

“With Lumio, we are able to raise the standard of care in remote clinics, bringing a level of assessment that was previously only possible within the hospital. I would definitely say it is a nifty device.”
Team structure and clinical workflow
Our hospital and outreach teams typically consist of around 10 staff members, including one ophthalmologist — myself. We work in a highly coordinated, almost conveyor‑belt‑style workflow, which allows us to manage large patient volumes efficiently.
Some team members focus on refractive error assessment, while I concentrate on cataract screening and anterior eye examinations to detect underlying disease. When a patient is identified as having a suspected cataract, we carry out on‑the‑spot blood tests for hepatitis B, hepatitis C, and HIV. This pre‑screening step is essential—it ensures the patient can be managed safely and placed on the correct surgical pathway, with appropriate hospital precautions in place.
Challenges in busy, resource limited environments
Time pressure is one of our greatest challenges, particularly during outreach clinics. We often see very large numbers of patients in a short period, and historically we relied on a basic ophthalmoscope as our primary diagnostic tool. This significantly limited both the depth of assessment and the range of conditions we could confidently diagnose on the spot.
More complex cases therefore needed referral back to the hospital, but referrals present their own difficulties. Many patients live far away and have limited or unreliable transport, and it can be challenging to convince them to make the journey—especially when symptoms do not yet feel severe.
Even within hospitals that are already stretched for resources, eye care is sometimes overlooked, as priority is often given to other, more immediately life‑threatening conditions. As a result, patients transferred between facilities for surgery or specialist care may simply disappear from the system. They are referred from one location to another and never return, leaving treatable eye conditions untreated.
These realities highlight how critical it is to achieve a broad eye assessment at the very first point of contact, particularly in outreach settings where follow‑up is never guaranteed.


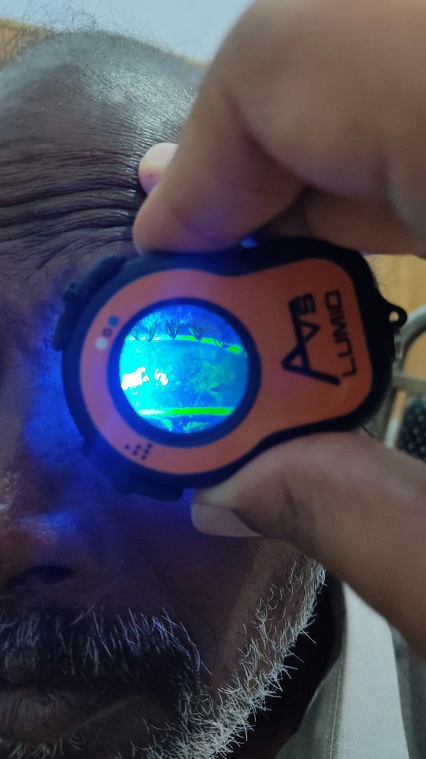
Eye tests being conducted with the Lumio (with and without) Fluorescein Filter in an outreach clinic setting
How Lumio has impoved our ability to provide care
Before using Lumio, our outreach work focused almost entirely on refractive error and identifying cataract patients. Anything beyond that was extremely difficult. Many borderline or complex cases—especially fungal infections, corneal scratches, and early surface pathology—were often sidelined simply because we lacked the equipment to assess them properly in the field. Sadly, this meant some patients with genuine pathology were not receiving the care they needed.
Lumio has fundamentally changed this for us. We are now able to look beyond cataracts and refractive error and give proper attention to conditions that were previously overlooked. It enables more detailed examinations, supports better‑informed clinical decisions, and gives us greater confidence—even in busy, high‑pressure outreach environments.
A key advantage of Lumio is its portability and speed. It is compact, practical, and ideally suited to rural and remote settings. In the past, our care was limited by what equipment we could realistically transport without risking damage. With Lumio, we are able to raise the standard of care in remote clinics, bringing a level of assessment that was previously only possible within the hospital. I would definitely say it is a nifty device.
Overall, Lumio has helped us move from basic screening to more comprehensive, meaningful eye care—even in some of the most challenging working conditions.
A "WOW" moment with Lumio
Previously, fluorescein examinations were only possible at the hospital using a slit lamp—we simply had no way to perform these assessments during outreach clinics.
My first real “wow” moment with Lumio came when I examined a severely infected patient using fluorescein in the field. The magnified view combined with the filter revealed the true scale of corneal damage immediately. It was clear that this patient needed urgent treatment.
That rapid insight made a huge difference. On days when we may see more than 500 patients, the ability to identify serious pathology quickly allows us to act immediately, provide medication on the spot, and ensure the patient leaves with treatment in hand. In cases like this, speed is not just convenient—it can make all the difference to the patient and their sight.

